TMJ Pain Treatment Singapore: Why Your Jaw Problem Lives in Your Neck
If your jaw clicks, locks, or aches daily, treating it in isolation rarely works. Night guards, massages, and passive chiropractic adjustments only mask the symptoms. They do not fix the structural cause.
Clinical evidence shows a direct link between cervical spine dysfunction, chronic neck pain, and temporomandibular joint disorders (TMD). When your neck lacks the muscular capacity to support your posture, your jaw muscles overwork to compensate. Standard, jaw-only approaches consistently fail because they ignore this relationship.
As an evidence-based TMJ chiropractor in Singapore, our approach to chiropractic treatment focuses on building long-term capacity in your neck so your jaw no longer has to overcompensate. Our active rehabilitation and clinical pilates programmes give you permanent, exercise-led independence from passive clinical maintenance.
Clinical Disruption
Clinical evidence shows that TMJ pain cannot be treated in isolation from neck pain. The cervical spine and temporomandibular joint function as interlinked biomechanical units. Restoring long-term, pain-free jaw function requires a global chiropractic strategy that addresses neck stabilisation and loading capacity.
TMJ Symptoms We Treat
Common Signs Your Jaw Problem Requires Neck Treatment
These symptoms indicate structural compensation patterns between your cervical spine and temporomandibular joint. Treating the jaw alone will not resolve them.
Jaw Clicking or Popping
Audible clicking when opening or closing your mouth, often accompanied by a catching sensation. Indicates disc displacement caused by altered jaw tracking from forward head posture.
Jaw Locking
Sudden inability to fully open or close your mouth. Results from disc dislocation when your mandible operates from a biomechanically compromised position due to weak cervical stabilisers.
Limited Mouth Opening
Difficulty opening beyond 35mm (measured between upper and lower front teeth). Caused by protective muscle guarding when your jaw attempts to function without adequate cervical support.
Teeth Grinding (Bruxism)
Unconscious clenching or grinding, particularly at night. Your jaw braces to stabilise your head when your deep cervical flexors cannot maintain proper alignment during sleep.
TMJ Headaches
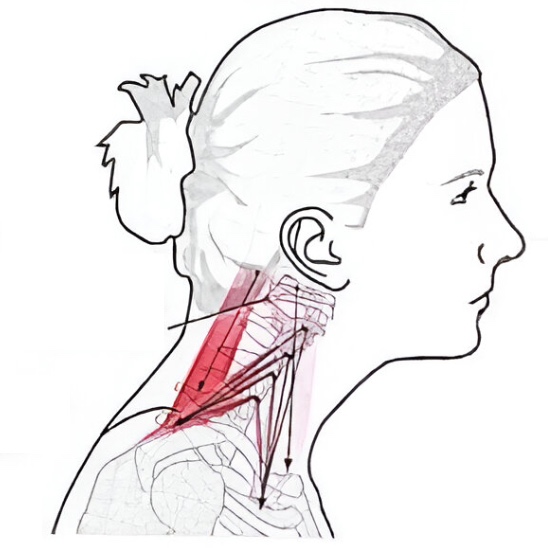
Pain radiating to temples, behind eyes, or across the forehead. Results from referred pain via the trigeminocervical complex when upper cervical nerves are chronically overloaded.
Ear Pain and Tinnitus
Ear fullness, ringing, or pain without infection. The TMJ sits directly anterior to the ear canal. Jaw misalignment from neck dysfunction creates pressure and referred symptoms.
Biomechanical Architecture
Why Your Neck Controls Your Jaw Function
Your jaw does not operate independently. It relies entirely on the structural stability your neck provides. When your deep cervical muscles lack the capacity to hold your head upright, your jaw compensates immediately.
Weak Neck Muscles Force Jaw Misalignment
The deep stabilisers in your neck anchor your skull. When these muscles cannot sustain proper head posture, your jaw tracking shifts to maintain balance. This compensation creates abnormal joint loading, leading to clicking, locking, and chronic pain.
Your temporomandibular joint is designed to glide smoothly through a precise arc of motion. That arc depends on your head sitting in optimal alignment above your spine. When forward head posture develops due to weak deep cervical flexors, your mandible is forced to operate from a compromised starting position. The disc inside the joint tracks incorrectly. The ligaments stretch unevenly. The muscles surrounding your jaw work overtime to stabilise what your neck should be controlling.
Your Brain Confuses Neck Pain for Jaw Pain
The nerve supply to your jaw and upper neck converge at the trigeminocervical complex in your brainstem. When your neck muscles are overloaded or weak, pain signals from both regions blend together. Your brain frequently misreads this input, making you feel severe jaw pain when the true dysfunction sits in your cervical spine.
This is not a theory. It is mapped anatomy. The trigeminal nerve, which supplies sensation to your face and jaw, shares processing space with the upper three cervical nerves. When your neck is in a state of chronic overload, these signals cross contaminate. You feel referred pain in your temples, behind your eyes, and deep in your jaw joint, even though the tissue generating the pain signal sits in your neck.
Breathing Patterns Reinforce the Dysfunction
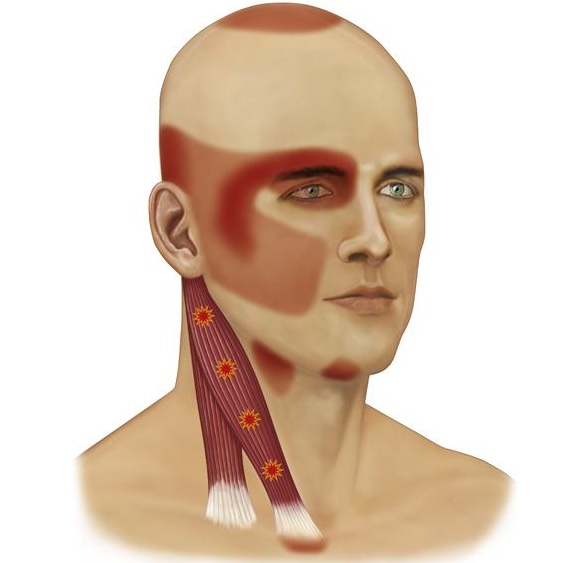
When your neck cannot support your head efficiently, your body recruits accessory breathing muscles to stabilise your skull. This means your scalenes, sternocleidomastoid, and upper trapezius work constantly, even at rest. These same muscles attach directly to your jaw or influence its position through fascial continuity.
Chronic upper chest breathing keeps your jaw in a state of low grade tension. Your masseter and temporalis muscles never fully relax because they are locked into a compensation pattern driven by your respiratory mechanics. Fixing your jaw means fixing your neck, and fixing your neck means restoring proper diaphragmatic breathing.
The Research Standard
The Research: Neck Training Beats Standard Jaw Therapy
A 2025 randomised controlled trial by Arslan et al., published in BMC Musculoskeletal Disorders, directly tested whether adding neck training improves TMJ outcomes beyond standard jaw care. The study divided 30 participants with TMJ disorders into two groups over eight weeks:
Control Group
Standard care including education about TMJ disorders and a home programme of Rocabado exercises (six specific jaw exercises targeting rest position, range of motion, and resistance training).
Cervical Stabilisation Group
The same standard care plus supervised cervical stabilisation training three times per week, focusing on deep neck flexor activation using pressure biofeedback and progressive exercises.
This is not an isolated finding. Multiple studies have demonstrated that manual therapy directed solely at the jaw produces short-term symptom relief but fails to create lasting structural change. The reason is obvious: you cannot build capacity by moving a joint passively. You build capacity by training the muscles that control that joint’s position.
The Results Were Clear
The control group receiving only jaw exercises showed minimal improvement. Cervical flexion and right lateral flexion improved slightly, but TMJ pain intensity, symptom severity, head posture, and neck muscle performance remained unchanged.
The group receiving cervical stabilisation training alongside jaw exercises demonstrated:
- ✓ Significantly lower resting jaw pain compared to the control group (mean difference with 81% effect size, p = 0.034)
- ✓ Marked improvement in TMJ symptom severity as measured by the Fonseca Anamnestic Index (p = 0.012)
- ✓ Measurable corrections in head posture via craniovertebral angle measurement (p = 0.040)
- ✓ Substantial gains in cervical mobility across all directions: flexion, extension, and lateral flexion (all p < 0.001)
- ✓ Superior cervical muscle performance compared to the control group (mean difference with 132% effect size, p = 0.001)
Systemic Critiques
What Standard TMJ Treatment Gets Wrong
Most TMJ treatment focuses on the site of pain rather than the source of dysfunction. This is why you have likely tried multiple approaches that provided temporary relief but no lasting resolution.
|
Dental Splints Mask the ProblemNight guards prevent tooth wear, but they do not address why you are clenching in the first place. Your jaw is bracing because of your overactive neck and jaw muscles that are not relaxing even when you sleep. A splint does protect the surface of your teeth but does not correct the underlying faulty motor pattern driving the grinding. |
Massage and Manual Therapy Provide Temporary ReliefReleasing tight jaw muscles feels good in the moment, but the relief disappears within hours or days because the structural cause remains untouched. Your masseter and temporalis muscles are overactive because they are compensating for weak deep cervical flexors. No amount of soft tissue work will change that relationship. |
Chiropractic Adjustments Do Not Build ResilienceClicking and popping your jaw back into place might restore short-term mobility and give some pain relief. However, it does nothing to train the muscles responsible for maintaining that position. The joint will return to its compensatory pattern the moment you leave the treatment table because the underlying capacity deficit still exists. |



Active Intervention Plan
How We Build Neck Capacity to Fix Your Jaw
We do not crack your neck. We do not massage your jaw. We teach you how to build the structural capacity your cervical spine needs so your jaw stops compensating.
|
1 Deep Cervical Flexor RetrainingWe use pressure biofeedback units to isolate and activate your deep neck stabilisers, particularly the longus colli and longus capitis. These muscles sit directly on the front of your cervical spine and are responsible for maintaining optimal head posture. Most people with chronic TMJ dysfunction have almost zero activation capacity in these muscles. They rely entirely on their superficial neck flexors, which creates chronic tension in the front of the neck and directly impacts jaw position. We train you to recruit these deep stabilisers in isolation first, then integrate them into functional movement patterns to immediately reduce the load on your jaw. |
2 Progressive Loading Under Real ConditionsYour neck must perform when you sit at a desk, carry bags, and move through your day. We progress you from basic floor exercises to upright, loaded movements using resistance bands, unstable surfaces, and dynamic head positioning. You will train your cervical spine to maintain stability while your jaw opens and closes, while you rotate your head, and while you perform upper body movements. This ensures your neck can handle real-world demand without offloading strain to your jaw. |
|
3 Neuromuscular ReprogrammingWe retrain the coordination between your neck and jaw so your brain stops defaulting to compensatory clenching and grinding. By addressing the faulty motor patterns at their source, we eliminate the underlying driver of your TMJ pain. This includes specific drills that teach your nervous system to dissociate jaw movement from neck tension. You will learn how to open your mouth, chew, and speak without triggering a protective bracing response in your cervical spine. |
4 Breathing Mechanics and Postural IntegrationWe assess and correct your breathing pattern. If you are locked into upper chest breathing, your accessory neck muscles will never relax, and your jaw will never release. We teach you how to restore diaphragmatic breathing while maintaining cervical stability. This dual approach ensures that your resting muscle tone normalises and your jaw can function without chronic background tension. |
Clinical Differentiation
TMJ Chiropractor vs Dentist: When to Choose Active Rehabilitation
Dentists manage occlusal issues and structural jaw problems. Chiropractors address the neuromuscular and postural drivers that cause your jaw to compensate. Different problems require different specialists.
When to See a Dentist for TMJ
- → Severe malocclusion (misaligned bite)
- → Structural jaw deformity
- → Severe disc displacement requiring surgery
- → Tooth wear requiring restorative work
- → Suspected infection or tumour
When to See a TMJ Chiropractor
- → Jaw pain with concurrent neck pain or stiffness
- → TMJ symptoms worsened by poor posture or desk work
- → Grinding/clenching without structural bite issues
- → Forward head posture with jaw clicking
- → Night guard provided temporary relief but symptoms returned
- → TMJ pain following whiplash or neck injury
Clinical Note: Many TMJ cases benefit from collaborative care. If your dentist has ruled out structural jaw problems but you still have pain, the dysfunction likely originates from cervical spine compensation. Active rehabilitation addresses the neuromuscular drivers that dental interventions cannot fix.
What to Expect in Your TMJ Assessment
Your initial consultation involves a detailed movement and capacity assessment of your cervical spine, not just your jaw. We do not guess. We test. The assessment gives us the objective data needed to design a targeted rehabilitation plan specific to your presentation.
Duration: 45–60 minutes
Location: Square One Active Recovery, Chinatown, Singapore
What to bring: Any imaging reports (X-rays, MRI) if available, list of current medications, comfortable clothing for movement assessment
Objective Evaluation Checklist
- ✓Quantifying deep cervical flexor output using handheld dynamometry
- ✓Assessing upper spine mobility and postural alignment across multiple planes
- ✓Evaluating accessory muscle recruitment and diaphragmatic integration
- ✓Analysing opening mechanics, end-range quality, and disc tracking
- ✓Mapping pain patterns originating from the trigeminocervical complex
What Happens After Your Assessment
If your assessment confirms cervical-driven TMJ dysfunction, we design a structured rehabilitation programme tailored to your capacity deficits. Most patients attend twice per week initially, then taper to once per week as they build autonomy with their exercise programme.
We do not prescribe indefinite care. Our objective is to restore structural capacity so you can manage your own recovery. Treatment duration depends on severity, but most patients achieve functional independence within 8–12 weeks of consistent training.
Common Questions
TMJ Treatment FAQ
Can TMJ be cured permanently?
TMJ dysfunction caused by cervical spine compensation can be permanently resolved by building structural capacity in your deep neck stabilisers. Once your neck can support your head without requiring jaw compensation, the mechanical drivers of TMJ pain are eliminated. This requires consistent exercise adherence, not passive maintenance.
How long does TMJ treatment take?
Treatment duration depends on severity, chronicity, and adherence to your exercise programme. Most patients achieve functional improvement within 4 to 6 weeks and reach independence within 8 to 12 weeks. Severe cases with significant structural compensation may require longer rehabilitation periods.
Do I need to stop wearing my night guard?
Continue wearing your night guard as prescribed by your dentist, especially if you have significant tooth wear. The night guard protects your teeth whilst we address the underlying neuromuscular cause of your clenching. Many patients find they no longer need the guard once their neck capacity improves, but this decision should be made with your dentist.
Will you crack or adjust my jaw?
No. We do not perform passive joint manipulations on the jaw or neck. Our approach is entirely exercise-based. We teach you how to build the muscular capacity that eliminates the need for external manual interventions.
Is this covered by insurance or Medisave in Singapore?
Chiropractic services are not currently claimable under Medisave. Some corporate and personal accident insurance plans do include chiropractic coverage. Please check your policy details. We provide detailed invoices for insurance claims where applicable.
I live in Raffles Place / Tanjong Pagar / CBD. How do I get to your clinic?
Square One Active Recovery is located in Chinatown, a 5-minute walk from Chinatown MRT (Exit E or G). We are walking distance from Raffles Place and Outram Park. HDB public car parks is available nearby.
What if I have both TMJ pain and chronic neck pain?
This is the typical presentation. TMJ pain and neck pain are almost always linked through the mechanisms described on this page. Addressing your cervical spine capacity will simultaneously resolve both issues because they share the same structural cause.